Diversion Dilema
With over 65% of America’s Emergency Departments reporting capacity issues, diverting ambulances has become common place. “To divert or not to divert?” is the questions often facing managers and administrators. Let us examine some quick facts.
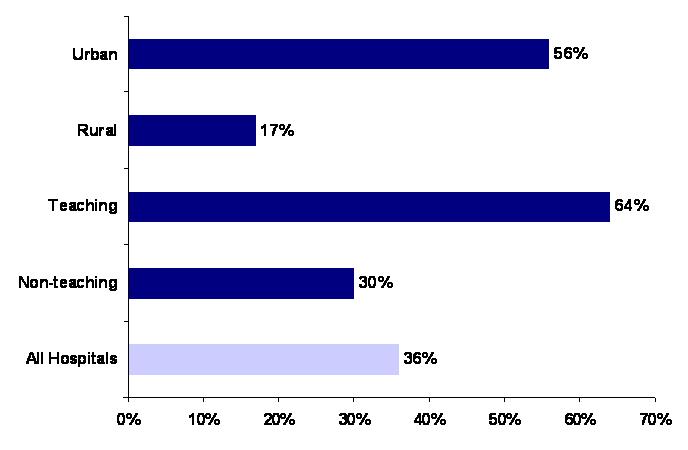
According to the AHA in 2007, over 56% of Urban hospitals reported diversions in 2007 (above)
Lack of staffed Critical care beds was cited as the number one reason for ambulance diversion
On average, approx. 15.5% patients arrive via ambulance
Is zero diversions possible?
With about 34 ambulances being sent to EDs around the US every minute, most administrators, even state and county officials have settled into status quo in most places. But there are some well documented and concerted efforts being made by a few EDs. Which brings us to the question, Is it really possible to have Zero diversions. The answer is a resounding Yes!!!. And this has been proven by Seattle’s best (no not the coffee company) . A policy has been passed in King County, WA to enforece zero diversions in Seattle area Emergency departments. The policy requires critically ill patients to be taken to the ‘hospital of their choice’ or the nearest hospital.
Facts from Seattle’s Zero Diversion policy
Hospital administrators agreed that throughput is a hospital problem not an ED problem
Setting guidelines and on pre-diversion targets is the key to reducing diversions
If a hospital is overloaded they can go on “ED saturation” two hours at a time and then get back to green and can only do this for a total of six hours in every 24
Rearranging staff for low and high acuity has helps tremendously
Reconfiguring the alert system is critical when changes are implemented